Table of Contents |
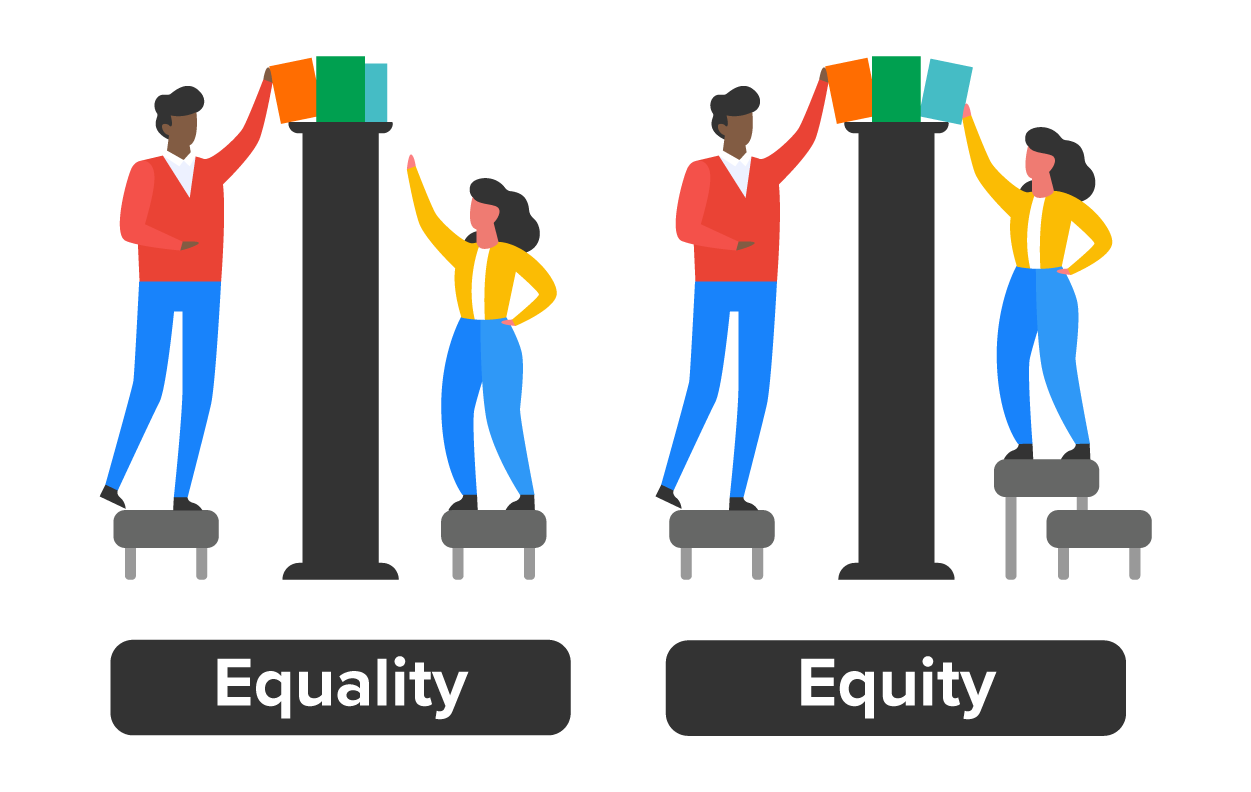
In the United States, there are groups of people who have an education or job training that ensures they are employed, make enough money to live in stable housing, have access to healthy food, own a car (or sometimes two), and have health insurance and therefore access to reliable and quality health care.
In other parts of the United States, some groups live the opposite of the life just described. They have little to no education or job training, relegating their employment opportunities to lower-paying jobs, which usually means a lack of money to afford reliable transportation, unstable housing, potentially living in a food desert where healthy food options are limited, and no health insurance. If they do live in poverty, they perhaps have access to Medicaid coverage, which means there are very few providers in their communities who accept their insurance. The quality of life between this group and the first group described is unequal.
The health outcomes of the first group will most likely be better over their lifetime than those of the second group. Striving for health equity seeks to balance the health outcomes of the second group closely with the first group in a manner that is sensitive to any differences in race, ethnicity, gender, sexual orientation, age, and SDOH.
This course has presented many scenarios wherein the race and culture of populations have been discussed in terms of equity. Populations can also be described by age and stage of life. For this lesson, health equity will be described through children and seniors, two populations also vulnerable to the impact of SDOH.
SDOH are key drivers of health inequities, and addressing them is fundamental to improving population health and ensuring that all individuals can achieve optimal health. The impact of the SDOH on health equity is significant and multifaceted. These determinants widen health disparities, which are unfair and avoidable differences in health status.
Addressing SDOH is crucial for achieving health equity. Interventions that address SDOH can lead to improvements in health outcomes and reductions in health disparities. This includes policies and programs that improve access to quality education, affordable housing, nutritious food, safe environments, and health care services (Centers for Disease Control and Prevention [CDC], 2023).
The CDC emphasizes that addressing SDOH is essential to overcoming persistent health disparities and achieving health equity. The CDC’s CORE Health Equity Strategy aims to incorporate health equity into all aspects of public health work, including science, programs, partnerships, and workforce engagement. The CDC strives to move beyond naming differences through “markers” such as race to identifying and addressing changeable “drivers” such as neighborhood conditions, housing, and access to quality health care (CDC, 2023).
As you have learned thus far, health disparities span regions, races, cultures, ethnicities, genders, ages, and sexual orientations. To dive deeper into the topic of social determinants, health disparities, and the achievement of health equity, we will focus on two age-related populations: children and seniors.

Health disparities in children are a significant concern, as they often reflect broader societal inequities. Children from disadvantaged groups, including those of color and living in poverty, experience worse health than their more privileged peers. Health inequity is largely attributed to differences in a child’s economic stability, education access and quality, health care access and quality, neighborhood and built environment, and social and community context (all SDOH). These disparities are not due to chance but are deeply rooted in societal and health care structures characterized by systemic racism. Systemic racism refers to the pervasive and deeply ingrained ways in which societies foster racial discrimination through mutually reinforcing systems.
IN CONTEXT
Racial Disparities
Historically, racially segregated housing policies have led to racial isolation. Black Americans often face disproportionate costs related to housing, limiting their opportunities, networks, education, wealth, health, and legal treatment (Banaji et al., 2021). Unequal access to quality education perpetuates racial disparities. Systemic racism affects school funding, curriculum, and teacher quality, impacting students of color. Racial bias affects access to social safety nets, loans, and credit. Students of color may encounter discriminatory practices in these areas. Racial disparities in health care access, treatment, and outcomes persist. Students of color also experience higher rates of chronic illnesses and inadequate medical care.
One SDOH discussed in the context of health disparities has been access to quality health care. Health systems greatly impact health disparities largely through varying levels of access to services, including services provided to children. Clinician decisions that are not always the same for everyone in a population (i.e., among children) can result in varying levels of quality of care provided. Clinicians’ decisions are often supported through decision-making tools such as the Clinical Practice Guidelines (CPGs), which can standardize care (widely used by health care professionals), improve outcomes, and reduce inequities. CPGs can, however, inadvertently exacerbate health disparities because clinicians use them differently, possibly providing greater quality care to advantaged, lower-risk groups over disadvantaged, higher-risk groups.
EXAMPLE
After the publication of CPGs for attention deficit hyperactivity disorder (ADHD), the health care providers of Black and Hispanic children were more likely to discontinue their patient’s medication and disengage from treatment. This pattern was possibly due to the suboptimal communication of the CPGs to providers of care to these populations. Lack of understanding about the CPGs may have resulted in provider problems addressing the parent’s or child’s concerns about taking medications (Yaeger et al., 2022).Children who face racism or discrimination may experience chronic stress, which negatively impacts their physical and mental health. Exposure to violence can also have lasting effects on a child’s well-being. These adverse experiences lived by children increase the likelihood of engaging in risky behaviors related to alcohol, smoking, and sexual risk and negatively influence health outcomes during adolescence and youth (Monroe et al., 2023).

When discussing the impact of SDOH on health disparities in children, we should consider children with special health care needs. SDOH like poverty and discrimination, including discrimination by some health care professionals and systems, are modifiable root causes of poor health outcomes. Children with disabilities often face various forms of discrimination that can significantly impact their lives. They may be segregated into separate schools or classes, not be given equal access to educational resources, or be denied necessary accommodations to learn effectively (Administration for Children & Families, n.d.).
The SDOH of neighborhood and built environment for children with disabilities includes many public spaces like schools, playgrounds, and transportation systems, which may lack the necessary adaptations, such as ramps or elevators, making them inaccessible to children who use wheelchairs. Information may not be in accessible formats, such as braille for children who are blind. Children with disabilities might experience bullying, isolation, and low expectations from society, which lead to a lack of confidence and self-esteem. Medical ableism (when a person is seen only through the lens of the disability and what they cannot do instead of what they can do) can manifest in health care settings where the needs of children with disabilities are not adequately met or their conditions are viewed solely as problems to be fixed.
Seniors comprise another age-related population that experiences the impact of the SDOH. SDOH that create health disparities (i.e., unstable housing, food insecurity, and lack of access to quality health care) among seniors can significantly impact their well-being. Health equity for seniors in public and community health involves ensuring seniors can attain their full potential without being disadvantaged by social or economic conditions. For example, studies have found that Alzheimer’s disease is more prevalent among the Black and Hispanic populations than other ethnic groups in the United States. Cultural differences and lack of health education on this disease contribute to these disparities. As in other populations, the quality of care for seniors is predicated on access to quality health services and stability in all other SDOH. Health inequities in seniors are found in residential segregation, discrimination, immigration, social mobility, work, retirement, education, income, and wealth, all impacting health and well-being (National Institute on Aging [NIA], 2020).
EXAMPLE
For seniors, health inequities related to the SDOH of housing can significantly impact their health. Over 10 million households headed by someone over 65 are cost-burdened, paying more than a third of their income on housing. Nearly three quarters of renters who earn less than $15,000 per year face this burden. Such financial strain can lead to cutbacks in food and medical care, affecting those with chronic health conditions (Molinsky, 2022).The SDOH of economic stability can significantly affect seniors, especially after they stop working and live life in retirement. Health disparities related to retirement, which is typically a time of changing economic stability, will potentially impact seniors’ health. Demographic trends and retirement income challenges lead to expanding economic risks among seniors. Many will require long-term care, but few purchase private insurance to support formal care expenses.

Assisted living, a home-like place where older adults get extra help with everyday tasks, and private home health care are often expensive and inaccessible to seniors with lower incomes and fewer assets. Consequently, there are more people of color in government-run nursing homes, as opposed to private, more expensive nursing homes, both as a percentage of the nursing home population and in relation to the overall racial and ethnic population. Nursing home residents tend to have more serious health conditions, such as chronic illnesses, cognitive impairment, or functional limitations and require round-the-clock medical attention and supervision. Nursing homes tend to serve more residents of color, who often report lower staffing levels, a higher number of deficiencies in supplies and other resources, and a lower quality of care than a resident of an assisted living facility might receive. Medicaid, insurance coverage for those living in poverty, is accepted by many nursing homes.
There are gender differences creating health disparities for seniors as well. Overall, women live longer than men, but they are more likely to develop osteoporosis or depressive symptoms. Men, on the other hand, are more prone to heart disease, cancer, or diabetes (NIA, 2020).
Promoting health equity for both children and seniors involves creating fair opportunities for everyone to reach their best health through equitable access to quality health services, education, housing, transportation, and child or senior care. Listening to diverse voices to understand their unique needs and challenges promotes health equity in these populations. Social justice can be promoted by collaborating with communities of color and vulnerable populations and advocating for policies that reduce health disparities and address health disparities (Calancie et al., 2022).
Source: THIS TUTORIAL WAS AUTHORED BY SOPHIA LEARNING. PLEASE SEE OUR TERMS OF USE.
REFERENCES
Administration for Children & Families. (n.d.). Health equity fact sheet. U.S. Department of Health & Human Services. www.acf.hhs.gov/equity/health-equity-factsheet
Banaji, M. R., Fiske, S. T., & Massey, D. S. (2021). Systemic racism: Individuals and interactions, institutions and society. Cognitive Research: Principles and Implications, 6, Article 82. doi.org/10.1186/s41235-021-00349-3
Calancie, L., Batdorf-Barnes, A., Verbiest, S., White, N., Lich, K. H., Corbie, G., Mullenix, A., & Cilenti, D. (2022). Practical approaches for promoting health equity in communities. Maternal and Child Health Journal, 26, Suppl. 1, 82–87. doi.org/10.1007/s10995-022-03456-9
Centers for Disease Control and Prevention. (2023, March 26). Health equity fact sheet. U.S. Department of Health & Human Services. www.cdc.gov/healthequity/core/fact-sheet/index.html
Molinksy, J. (2022, August 18). Housing for America’s older adults: Four problems we must address. Joint Center of Housing Studies of Harvard University. www.jchs.harvard.edu/blog/housing-americas-older-adults-four-problems-we-must-address
Monroe, P., Campbell, J. A., Harris, M., & Egede, L. E. (2023). Racial/ethnic differences in social determinants of health and health outcomes among adolescents and youth ages 10–24 years old: A scoping review. BMC Public Health, 23, Article 410. doi.org/10.1186/s12889-023-15274-x
National Institute on Aging. (2020, May 20). Goal F: Understand health disparities related to aging and develop strategies to improve the health status of older adults in diverse populations. National Institutes of Health. www.nia.nih.gov/about/aging-strategic-directions-research/goal-health-disparities-adults
Yaeger, J. P., Alio, A. P., & Fiscella, K. (2022). Addressing child health equity through clinical decision-making. Pediatrics, 149(2), e2021053698. doi.org/10.1542/peds.2021-053698