Recall that erythrocytes, commonly known as red blood cells (RBCs), are by far the most commonly formed element in blood: A single drop of blood contains millions of RBCs and just thousands of leukocytes (white blood cells, WBCs). Specifically, males have about 5.4 million RBCs per microliter (µL) of blood, and females have approximately 4.8 million per µL. In fact, erythrocytes are estimated to make up about 25% of the total cells in the body. As you can imagine, they are quite small cells, with a mean diameter of only about 7–8 micrometers (µm). The primary functions of RBCs are to pick up inhaled oxygen from the lungs and transport it to the body’s tissues as well as to pick up some carbon dioxide waste at the tissues and transport it to the lungs for exhalation.
1. Shape and Structure of Erythrocytes
Mature, circulating erythrocytes have few internal cellular structural components, having ejected them during development. They lack a nucleus, endoplasmic reticula, and a Golgi apparatus, which means they cannot produce or process proteins or lipids. They lack mitochondria, which means they rely on anaerobic respiration for ATP production and therefore do not use any of the oxygen they transport. RBCs do, however, contain some structural proteins that help the blood cells maintain their unique structure and enable them to change their shape to squeeze through capillaries.
Shape of Red Blood Cells—Erythrocytes are biconcave discs with very shallow centers. This shape optimizes the ratio of surface area to volume, facilitating gas exchange. It also enables them to fold up as they move through narrow blood vessels.
Erythrocytes have a unique shape called a biconcave disc; that is, they are plump at their periphery and very thin in the center. Since they lack most organelles, there is more interior space for the presence of the hemoglobin molecules that, as you will see shortly, transport gases. The biconcave shape also provides a greater surface area across which gas exchange can occur, relative to its volume; a sphere of a similar diameter would have a lower surface area to volume ratio.
In the capillaries, the oxygen carried by the RBCs can diffuse into the plasma and then through the capillary walls to reach the cells, whereas some of the carbon dioxide produced by the cells as a waste product diffuses into the capillaries to be picked up by the RBCs. Capillary beds are extremely narrow, slowing the passage of the RBCs and providing an extended opportunity for gas exchange to occur.
However, the space within capillaries can be so small that despite their own small size, RBCs may have to fold in on themselves if they are to make their way through. Fortunately, their structural proteins like spectrin are flexible, allowing them to bend over themselves to a surprising degree, then spring back again when they enter a wider vessel. In wider vessels, RBCs may stack on top of one another much like a roll of coins, forming a rouleau (plural = rouleaux), from the French word for “roll.”
Rouleaux—To pass through small blood vessels such as capillaries, erythrocytes form stacks called rouleaux.
2. Hemoglobin
Hemoglobin is a large molecule made up of proteins and iron. It consists of four folded chains of a globin protein, designated alpha 1, alpha 2, beta 1, and beta 2 (see label a, below). Each of these globin molecules is bound to a red pigment molecule called heme, which contains an ion of iron (Fe²⁺) (see label b, below).
Hemoglobin—(a) A molecule of hemoglobin contains four globin proteins, each of which is bound to one molecule of the iron-containing pigment heme. (b) A single erythrocyte can contain 300 million hemoglobin molecules, and thus more than 1 billion oxygen molecules.
Each iron ion in the heme can bind to one oxygen molecule; therefore, each hemoglobin molecule can transport four oxygen molecules. An individual erythrocyte may contain about 300 million hemoglobin molecules and therefore can bind to and transport up to 1.2 billion oxygen molecules.
In the lungs, hemoglobin picks up oxygen, which binds to the iron ions, forming oxyhemoglobin. The bright red, oxygenated hemoglobin travels to the body tissues, where it releases some of the oxygen molecules, becoming darker red deoxyhemoglobin. Oxygen release depends on the need for oxygen in the surrounding tissues, so hemoglobin rarely, if ever, leaves all of its oxygen behind.
In the capillaries, carbon dioxide (CO₂) enters the bloodstream. Approximately 76% dissolves in the plasma, some remaining as dissolved CO₂, and the remainder forming bicarbonate ions. About 23%–24% of it binds to the amino acids in hemoglobin, forming a molecule known as carbaminohemoglobin. From the capillaries, the hemoglobin carries CO₂ back to the lungs, where it releases it for the exchange of oxygen.
did you know
Your blood is red because of hemoglobin. But did you know that not all blood is red?
As you have learned, each of the four globin proteins of hemoglobin contains a heme, which is a red pigment containing the atom iron. When bound by oxygen (oxyhemoglobin), it is a bright red color. When not bound by oxygen (deoxyhemoglobin), it is a deep or dark red.
The table below describes some of the different molecules that result in differently colored blood in other organisms.
The Chemistry of the Different Colors of Blood
Red
Blue
Green
Violet
Humans and the majority of other vertebrates
Spiders, crustaceans, some mollusks, octopuses, and squids
Some segmented worms, some leeches, and some marine worms
Marine worms including peanut worms, penis worms, and brachiopods
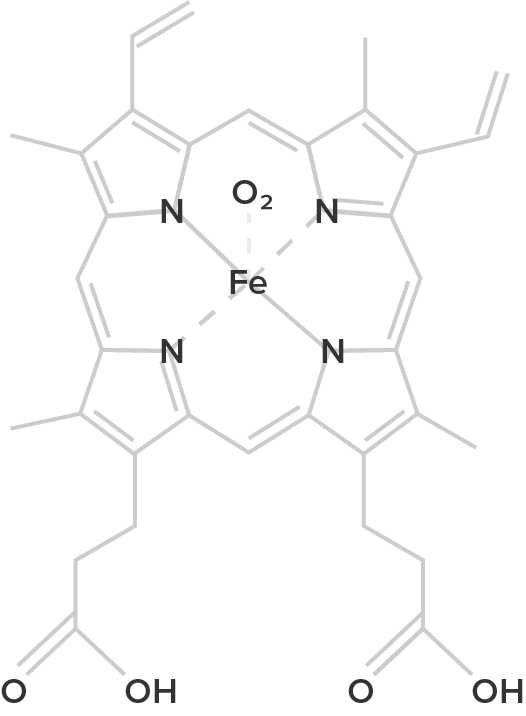
Hemoglobin
Heme B
(oxygenated form)
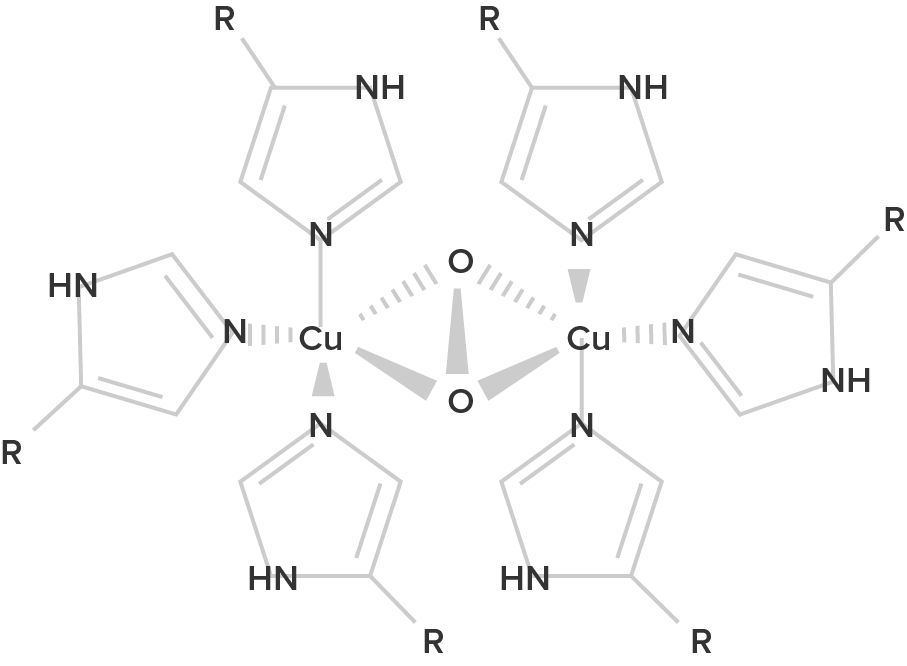
Hemocyanin
Hemocyanin B
(oxygenated form; R = histidine residues)
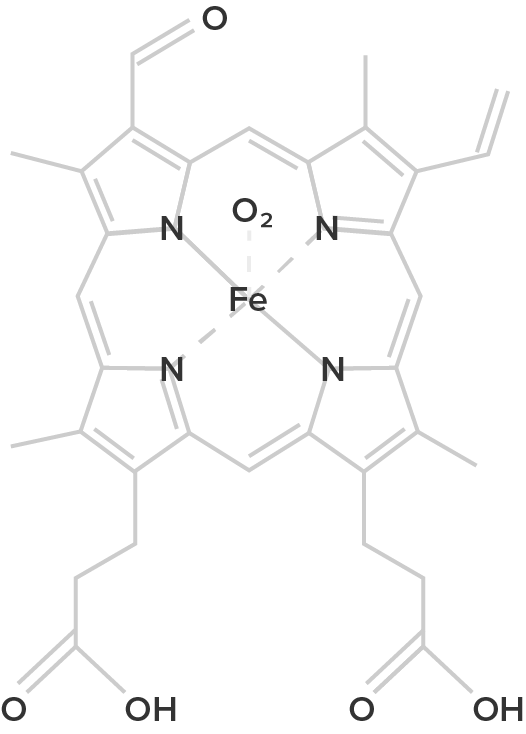
Chlorocruorin
Chlorocruorin
(oxygenated form)
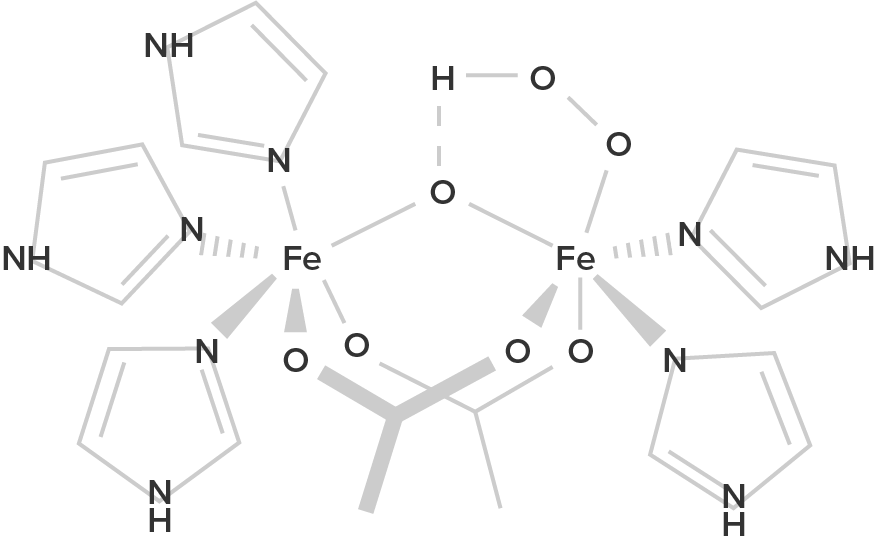
Hemerythrin
Hemerythrin
(oxygenated form)
Hemoglobin is a protein found in the blood, built up from subunits containing “hemes.” These hemes contain iron, and their structure gives blood its red color when oxygenated. Deoxygenated blood is a deep red color—not blue!
Unlike hemoglobin, which is bound to red blood cells, hemocyanin floats free in the blood. Hemocyanin contains copper instead of iron. When deoxygenated, the blood is colorless, but when oxygenated, it has a blue coloration.
Chemically similar to hemoglobin; the blood of some species contains both hemoglobin and chlorocruorin. Light green when deoxygenated, it is green when oxygenated, although when more concentrated, it appears light red.
Hemerythrin is only 1/4 as efficient at oxygen transport when compared to hemoglobin. In the deoxygenated state, hemerythrin is colorless, but it imparts a violet-pink color when oxygenated.
Changes in the levels of RBCs can have significant effects on the body’s ability to effectively deliver oxygen to the tissues. This can occur for many reasons, including reduced hematopoiesis, increased RBC damage or death, insufficient hemoglobin, and more. In determining the oxygenation of tissues, the value of the greatest interest in healthcare is the percent saturation—that is, the percentage of hemoglobin sites occupied by oxygen in a patient’s blood. Clinically, this value is commonly referred to simply as “percent sat.”
Percent Saturation—A pulse oximeter uses light to detect the oxygen saturation of hemoglobin through the skin.
Percent saturation is normally monitored using a device known as a pulse oximeter, which is applied to a thin part of the body, typically the tip of the patient’s finger. Normal pulse oximeter readings range from 95%–100%. Lower percentages reflect hypoxemia, or low oxygen levels in the blood. The term hypoxia is more generic and simply refers to low oxygen levels in the body. Oxygen levels are also directly monitored from free oxygen in the plasma, typically following an arterial stick. When this method is applied, the amount of oxygen present is expressed in terms of partial pressure of oxygen, or simply P₀₂ or PO2, and it is typically recorded in units of millimeters of mercury, mm Hg.
IN CONTEXT
Populations dwelling at high elevations, with inherently lower levels of oxygen in the atmosphere, naturally maintain a hematocrit higher than people living at sea level. Consequently, people traveling to high elevations may experience symptoms of hypoxemia, such as fatigue, headache, and shortness of breath, for a few days after their arrival. In response to hypoxemia, the kidneys secrete EPO to step up the production of RBCs until homeostasis is achieved once again.
To avoid the symptoms of hypoxemia, or altitude sickness, mountain climbers typically rest for several days to a week or more at a series of camps situated at increasing elevations to allow EPO levels and, consequently, RBC counts, to rise. When climbing the tallest peaks, such as Mt. Everest and K2 in the Himalayas, many mountain climbers rely upon bottled oxygen as they near the summit.
Acclimatization—Mount Everest south base camp in Nepal sits at 5,364 meters (17,598 feet, 3.3 miles). Hikers typically spend time at base camp before making their ascent in order to adapt to the new altitude which includes increasing the number of circulating erythrocytes to deliver adequate oxygen to the body.
terms to know
Hemoglobin
A large molecule found in erythrocytes that binds and transports oxygen and carbon dioxide.
Heme
An iron-containing, red pigment that forms a part of hemoglobin and binds oxygen.
Oxyhemoglobin
Hemoglobin with oxygen bound to it.
Deoxyhemoglobin
Hemoglobin without oxygen bound to it.
Carbaminohemoglobin
Hemoglobin with carbon dioxide bound to it.
Hypoxemia
Low levels of oxygen in the blood.
Hypoxia
Low levels of oxygen in the body.
3. Lifecycle of Erythrocytes
Erythrocytes, or red blood cells (RBCs), account for approximately 70% of the cells in the adult human body, and each only survives up to 120 days. Given the quick turn around and significant importance for the survival of the body, it is important to understand their production, existence, and removal.
The erythrocyte lifecycle is summarized in the figure below.
Erythrocyte Lifecycle—Erythrocytes are produced in the bone marrow and sent into the circulation. At the end of their lifecycle, they are destroyed by macrophages, and their components are recycled.
3a. Production and Existence
Recall that erythrocytes are produced, like all formed elements, in the overarching process of hematopoiesis in the bone marrow. In this process, a hematopoietic stem cell is subjected to hematopoietic growth factors and differentiates into a specific formed element. Each formed element follows a different pathway through hematopoiesis. Hematopoietic stem cells subjected to erythropoietin (EPO) will become RBCs in a specific process known as erythropoiesis.
Erythropoiesis—Hematopoietic stem cells differentiate into erythrocytes through the process of erythropoiesis, a portion of the larger hematopoiesis process.
To become an RBC, a hematopoietic stem cell must first differentiate into a myeloid stem cell and then commit to erythropoiesis by becoming a proerythroblast. Once committed to erythropoiesis, a proerythroblast goes through many specific changes, which include the production of hemoglobin and the expulsion of its nucleus and most of its organelles. These changes from proerythroblast to reticulocyte primarily occur in the bone marrow and can be expedited by the presence of EPO to more quickly increase the number of RBCs in the blood (Hattangadi, et al. 2011).
During the first day or two that it is in circulation, an immature red blood cell, known as a reticulocyte, will still typically contain remnants of organelles. Reticulocytes should comprise approximately 1%–2% of the RBC count and provide a rough estimate of the rate of RBC production, with abnormally low or high rates indicating deviations in the production of these cells. These remnants, primarily of networks (reticulum) of ribosomes, are quickly shed, and a mature RBC remains.
As you know, RBCs function to transport oxygen and carbon dioxide throughout the body. Since they lack the ability to produce proteins, make repairs, or generate significant amounts of ATP, their life is short, at approximately 120 days.
try it
Directions: Review the scenario and answer the question below.
Erythrocytes make up approximately 70% of the cells in the adult human body, which contains a total of around 30 trillion cells. If they live for only 120 days, then the body must replace them all in that time frame.
Production of red blood cells in the marrow occurs at the staggering rate of more than 2 million cells per second. For this production to occur, a number of raw materials must be present in adequate amounts. These include the same nutrients that are essential to the production and maintenance of any cell, such as glucose, lipids, and amino acids. However, RBC production also requires several trace elements:
Iron. We have said that each heme group in a hemoglobin molecule contains an ion of the trace mineral iron. On average, less than 20% of the iron we consume is absorbed. Heme iron, from animal foods such as meat, poultry, and fish, is absorbed more efficiently than non-heme iron from plant foods. Upon absorption, iron becomes part of the body’s total iron pool. The bone marrow, liver, and spleen can store iron in the protein compounds. When EPO stimulates the production of RBCs, iron is released from storage and carried to the red marrow, where it attaches to RBC precursors.
Copper. A trace mineral, copper is a component of two plasma proteins, hephaestin and ceruloplasmin. Without these, hemoglobin could not be adequately produced. Located in the intestines, hephaestin enables iron to be absorbed by intestinal cells. Ceruloplasmin transports copper. In a state of copper deficiency, the transport of iron for heme synthesis decreases, and iron can accumulate in tissues, where it can eventually lead to organ damage.
Zinc. The trace mineral zinc functions as a coenzyme that facilitates the synthesis of the heme portion of hemoglobin.
B vitamins. The B vitamins folate and vitamin B₁₂ function as coenzymes that facilitate DNA synthesis. Thus, both are critical for the synthesis of new cells, including RBCs.
terms to know
Erythropoiesis
The production of erythrocytes.
Reticulocyte
An immature erythrocyte.
3b. Recycling
As you have learned, erythrocytes live up to 120 days in the circulation. At the end of this time, RBCs are removed from functional use in one of two ways. Some cells rupture during circulation in a process known as hemolysis (haima, blood; lysis, to cut). Their cell contents are released into the blood. Most worn-out RBCs, however, are removed by a type of phagocytic cell (cells that ingest large particles and dead or dying cells) called a macrophage, located primarily within the bone marrow, liver, and spleen. The components of the degraded RBCs’ hemoglobin are further processed as follows:
Globin, the protein portion of hemoglobin, is broken down into amino acids, which can be sent back to the bone marrow to be used in the production of new RBCs. Hemoglobin that is released by hemolysis is broken down to alpha and beta chains in the blood, which are then removed from circulation by the kidneys.
The iron contained in the heme portion of hemoglobin may be stored in the liver or spleen or carried to the red bone marrow for recycling into new RBCs.
The non-iron portion of heme is degraded into the waste product biliverdin, a green pigment, and then into another waste product, bilirubin, a yellow pigment. Bilirubin binds to albumin and travels to the liver, which uses it in the manufacture of bile, a compound released into the intestines to help digest fats. In the large intestine, bacteria break the bilirubin apart from the bile and convert it to urobilinogen, a colorless pigment, and then into stercobilin, a brown pigment. It is then eliminated from the body in the feces (poop), which are brown. The kidneys also remove any circulating bilirubin and other related metabolic byproducts such as urobilinogen and secrete them into the urine. When urobilinogen is oxidized by exposure to air outside the body, it turns into urobilin, a yellow pigment.
The breakdown pigments formed from the destruction of hemoglobin can be seen in a variety of situations. At the site of an injury, biliverdin from damaged RBCs produces some of the dramatic colors associated with a bruise.
Bruise—Over time, a bruise will display multiple different colors based on the oxygen status of hemoglobin and production of its breakdown products.
As noted, the liver processes bilirubin into bile. However, if the liver function decreases, bilirubin can build up and not be efficiently removed from the blood circulation. In this case, the body assumes a yellowish tinge, especially the white sclera of the eyes, which is a condition known as jaundice.
Jaundice—Decreased liver function will cause bilirubin, a yellow pigment byproduct of hemoglobin breakdown, to build up in the blood, which causes the body to yellow. The first symptom is typically seen in the white sclera of the eyes.
Appropriately, this discoloration of the eyes and/or body indicates an issue with liver function. While bilirubin may be beneficial in protecting against oxidative stress at mildly elevated levels (Bulmer, et al. 2008), it is a neurotoxin and can cause severe neurological damage at high levels.
IN CONTEXT
A significant number of newborn babies develop jaundice in their first few days or weeks after birth. Breast milk normally helps newborns dislodge the waste built up in their large intestine, which contains significant deposits of bilirubin. If the waste is not quickly removed, the bilirubin can be reabsorbed back into the blood. Given a baby’s development, the neurotoxicity of bilirubin is a major concern.
However, the treatment is simple—UV light. UV light helps to alter bilirubin so that it is no longer a neurotoxin and can be more easily removed by the kidneys. Hospitals use special UV lights while parents may be advised to expose newborns to some level of natural sunlight throughout the day.
Phototherapy—A newborn baby with hyperbilirubinemia is subjected to a blue UV light to help reduce bilirubin levels.
terms to know
Hemolysis
The rupturing of an erythrocyte in the blood.
Macrophage
A phagocytic cell.
Biliverdin
A green pigment; a byproduct of heme breakdown.
Bilirubin
A yellow pigment; a byproduct of heme breakdown incorporated by the liver into bile.
Stercobilin
A brown pigment; a byproduct of heme breakdown.
Urobilin
A yellow pigment; a byproduct of heme breakdown.
Bruise
Localized bleeding under the skin due to damaged blood vessels.
Jaundice
Yellowing of the body due to decreased liver function and increased bilirubin in the blood.
summary
In this lesson, you learned about the structure, function, production, and recycling of erythrocytes. You first learned about the unique shape and structure of erythrocytes. You also learned about hemoglobin and how it allows erythrocytes to transport gases throughout the body. Finally, you learned about the lifecycle of erythrocytes. You explored the process by which their production and existence is possible. You also learned about how the body goes about recycling the components of erythrocytes and how those components are used in the body.


 A molecule of hemoglobin contains four globin proteins, each of which is bound to one molecule of the iron-containing pigment heme. (b) A single erythrocyte can contain 300 million hemoglobin molecules, and thus more than 1 billion oxygen molecules.")
 Humans and the majority of other vertebrates
Humans and the majority of other vertebrates
 Spiders, crustaceans, some mollusks, octopuses, and squids
Spiders, crustaceans, some mollusks, octopuses, and squids
 Some segmented worms, some leeches, and some marine worms
Some segmented worms, some leeches, and some marine worms
 Marine worms including peanut worms, penis worms, and brachiopods
Marine worms including peanut worms, penis worms, and brachiopods





. Hikers typically spend time at base camp before making their ascent in order to adapt to the new altitude which includes increasing the number of circulating erythrocytes to deliver adequate oxygen to the body.")
