Table of Contents |

In this lesson, you will learn about physical exams. The physical exam is a component of the overall patient assessment. In this case, the physician physically touches the patient to perform their assessment. This term can also be used to describe a specific type of medical appointment that is sometimes called a wellness check, routine exam, preventative care, or annual physical (AdventHealth, 2025; Cleveland Clinic, 2023).
Physical exams are not the same as a sports physical, which is focused on specific systems (height, weight, muscles, bone health, vision, and hearing). Instead, they focus on general health. A larger physical exam, such as an annual exam, typically involves an examination of physical appearance, review of vital signs (like pulse), and discussion of current medication (Cleveland Clinic, 2023).
In this lesson, you will learn more about assessing a patient and conducting a physical exam.
A comprehensive physical exam includes two major components: a general survey and system-specific assessments (meaning assessments of specific body systems). Here is a summary of related terms:
- Inspection – Visual observation of body features and movements
- Palpation – Using hands to feel organs, masses, or tenderness
- Percussion – Tapping to assess underlying structures (e.g., lungs, abdomen)
- Auscultation – Listening to internal sounds using a stethoscope
Useful terms to describe the findings of a physical exam include: tenderness, mass, distension, rigidity, crepitus, and effusion. Crepitus is a crackling or popping heard in a joint or in the lungs (Verywell Health, 2025).
The standard vital signs are documented, which include:
- Temperature (Temp)
- Heart Rate (HR) / Pulse
- Respiratory Rate (RR)
- Blood Pressure (BP)
- Oxygen Saturation (O2 Sat)
There are specific terms and abbreviations to know for different body systems.
EXAMPLE
A neurological assessment may include assessments of cranial nerves, motor strength, sensation, reflexes, and gait and coordination.HEENT refers to head, eyes, ears, nose, and throat. PERRLA means pupils equal, round, reactive to light and accommodation. TM is the tympanic membrane.
A useful abbreviation for the musculoskeletal system is ROM (range of motion).
During the initial assessment, it is important for a clinician to pay attention so that they can note all relevant observations that may affect diagnosis and treatment.
A patient history provides detailed information about their past medical experiences and the progression of the current problem. A comprehensive medical history should thoroughly document important diagnoses, procedures such as surgeries, and relevant family medical history (Nichol et al., 2024).
The patient history is often obtained through an informal conversation. However, the following components are important: medical history, surgical history, family history, social history (e.g., eating habits, nutrition, use of substances and alcohol), allergy history, medication history, and any specialized history relevant to the current concern (e.g., reproductive history; Nichol et al., 2024).
In a patient history, you will often see the following terms:
- Chief complaint (CC): The reason that the patient is seeking medical care
- History of present illness (HPI): A detailed description of the progression of the CC
- Review of systems (ROS): A description of the status of major body systems (the level of detail varies; Goldberg, n.d.)
There are also some commonly encountered acronyms related to physical exams that are useful to know.
- WNL – Within normal limits
- NAD – No acute distress
- NT/ND – Non-tender / non-distended
- BS – Bowel sounds
- RRR – Regular rate and rhythm
- DOE – Dyspnea on exertion
- SOB – Shortness of breath
You will also often encounter the abbreviation EMR, which means electronic medical record.
With all of these abbreviations, make sure that there is no possibility of confusion.
EXAMPLE
You previously saw that SOB could be confused as shortness of breath or side of bed. In an assessment of respiration, SOB would clearly mean shortness of breath.A clinician should pay attention to a patient’s appearance. It is important to notice things like skin color, including signs like paleness or cyanosis, which can suggest a lack of oxygen. Yellowing of the skin and sclera (jaundice) often indicates a liver abnormality. A patient who is not well-groomed or well-dressed could be struggling to be able to perform activities of daily living. A patient who appears uncomfortable could be struggling with pain or difficulty breathing.

Another vital observation is the behavior of the patient. Unexpected or atypical behaviors can indicate anything from psychiatric conditions, hypoxic states, infections, or neurological complications. Restlessness can be a sign of hypoxia. Other signs of hypoxia and respiratory distress include posturing such as leaning forward with hands on a table, lethargy, inability to ambulate, accessory muscle use, cyanosis, and pallor. A depressed individual may avoid eye contact and have a flat affect.
Determining the patient’s age, gender, and culture can be helpful in providing care. Many diseases and conditions are linked to biological sex and ethnic backgrounds. These topics can be sensitive, and best practice standards require asking the patient about them directly, and asking about patient preferences, instead of making assumptions. It is appropriate to directly ask patients about their specific cultural practices as relevant to the medical assessment.
Assessments of growth and development are essential to determine if a patient is progressing through the stages of life as expected and are measured throughout the life span. A patient’s growth is obtained through anthropometric measurements and compared to normal values for the individual’s age. Development is assessed by both observation and interviewing. Development involves the mastery of developmental tasks in gross motor skills, fine motor skills, speech, and social skills. If there is a concern that development is delayed, typically in children, specific tests can be used.

Assessing the cognitive status includes the patient’s level of consciousness, facial expression, speech, and mental acuities. If abnormalities exist, a more in-depth mental examination is needed. The first aspect of cognitive assessment is determination of the patient’s level of consciousness, or their level of awareness and arousal. Assessing and addressing a patient’s pain is also imperative because pain can interfere with the patient’s ability to engage with the nurse’s cognitive assessment. Patients who are alert and with intact cognition should be able to provide the following information:
Other descriptive terms for a patient’s level of consciousness are lethargic, obtunded, sedated, and comatose. Lethargic means the individual is fatigued, drowsy, and difficult to arouse. Obtunded is used for patients with severe lethargy and lessened response to stimuli. Patients are considered sedated if they are receiving medications to sedate them (sedatives). A comatose patient is one who is completely unarousable and has no response to stimuli.
The Glasgow Coma Scale (GCS) is a scale that is frequently used to measure a patient’s level of consciousness by assessing eye opening, verbal response, and motor response. The highest possible GCS score is fifteen, and the lowest is three. A score of fifteen is considered normal, while a score of eight or less is consistent with a severe head injury.
You have already encountered many of the procedures and instruments used for standard patient assessments. Assessment often involves documenting vital signs, which are temperature, pulse, respiratory rate, blood pressure, and oxygen saturation. A vital sign is a marker of physiological homeostasis, so they are essential in the analysis of monitoring patient progress. When possible, vital signs are gathered during the initial encounter with the patient to establish a baseline and routinely thereafter, according to condition, to assess disease progression or resolution. Below, you will learn more about measuring temperature, pulse, respiratory rate, and blood pressure.
Temperature is an important vital sign to measure. It provides clues to other body systems, and or processes for maintaining homeostasis, such as the presence or absence of an infection, a functioning hypothalamus, and an effective integumentary system. Various types of thermometers are available to take temperature measurements. These include oral, rectal, tympanic, and axillary thermometers.
The oral thermometer is the most common type used to measure temperature and yields an average normal result of 98.6°F (37°C). These thermometers measure temperature through contact with the sublingual region, under the tongue.
The figure below shows an oral thermometer.
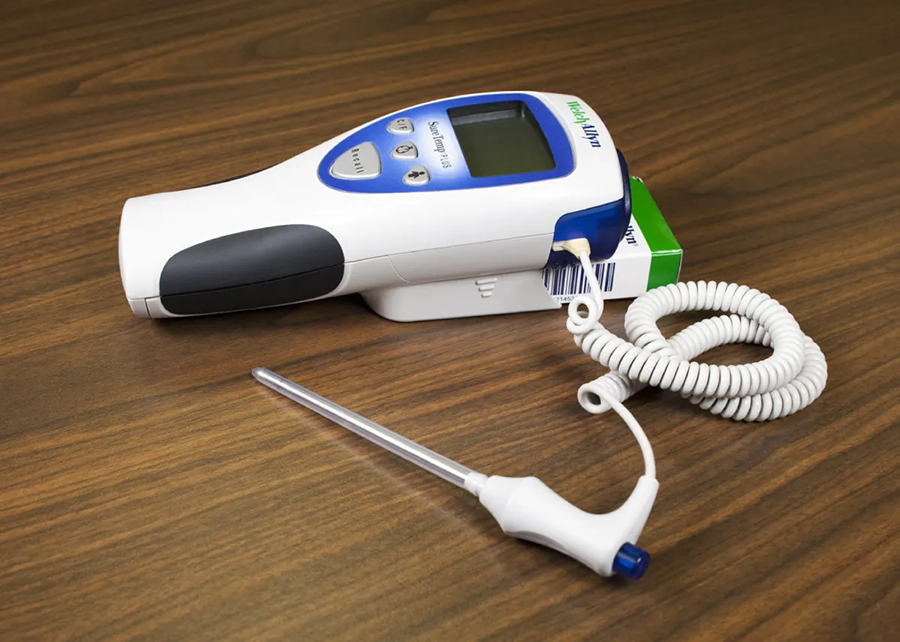
The rectal thermometer is the most accurate but also the most invasive type of thermometer. For this reason, it is generally only used for infants and in critical situations. The thermometer below can be used for multiple routes, but the correct color-coded probes and covers must be used to adapt it for a specific route (such as rectal).
Obtaining an axillary temperature is minimally invasive since it only requires contact with the skin of the axilla region under the arm, but its results are generally 1°F (0.6°C) lower than oral measurements.
The tympanic thermometer obtains a temperature through a probe inserted in the ear, and its results are slightly higher than an oral reading.
The photo below shows a tympanic thermometer.

Palpating the pulse is another aspect of obtaining vital signs. Pulse and respiration are especially important to assess in emergency situations. Palpation of the peripheral pulses, those arteries farthest away from the heart, provide information about the heart rate, rhythm, and strength.
The stroke volume (SV) represents the amount of blood pumped by the left ventricle with each contraction. Heart rate and stroke volume determine cardiac output, which is the total amount of blood ejected by the heart into circulation in one minute, measured in liters. If the stroke volume is significantly increased, the heart rate can decrease as the same cardiac output is achieved. Stroke volume and cardiac output are inversely related.
Obtaining respirations, or breathing pattern, is another aspect of checking vital signs. One respiration is complete inspiration and exhalation. Obtaining the respiratory rate verifies that the patient is breathing and not in respiratory distress while also ensuring the rhythmic exchange of oxygen and carbon dioxide. For routine vital sign assessment, the respiratory rate is obtained by observing the rise and fall of the chest immediately following the pulse check.
The efficiency of the respiratory system is assessed not only through obtaining the respiratory rate but also by assessing the oxygen saturation of the blood, abbreviated as SpO₂. To assess if blood, is being adequately oxygenated, a pulse oximeter is used.
The normal adult respiratory rate is 12 to 20 breaths per minute. When the respiratory rate exceeds 20 breaths per minute, tachypnea occurs. When the rate is below 12 breaths per minute, bradypnea occurs. A lower-than-normal respiratory rate is also called respiratory depression, a side effect of anesthetics and opioids.
Blood pressure must be measured to ensure the pressure is adequate to perfuse the body and not too great to rupture the blood vessels. It is measured using a sphygmomanometer. It consists of two numbers, a higher systolic and lower diastolic, and is reported as a fraction with the systolic on top and the diastolic on the bottom. Systole is the pressure of blood during contraction of the left ventricle. Diastole is the pressure of the blood when the ventricles are at rest and filling.
The figure below shows different sizes of blood pressure cuffs. In the top row, from left to right, the cuff sizes are bariatric, adult large, and adult. In the bottom row, the cuff sizes are child, infant, and neonate.

The difference between the systolic and diastolic blood pressure is the pulse pressure, which should normally be about 40 mm Hg. A narrowed pulse pressure is defined as a pulse pressure less than 25 percent of the systolic blood pressure (i.e., 110/85). A widened pulse pressure is defined as more than 100 mm Hg (i.e., 174/69).
Shock occurs when there is insufficient blood reaching the tissues, which can be fatal. This can occur due to low blood pressure from blood loss or when blood is shunted from the periphery to major organs in an emergency.
| Types of Shock | Description | Causes |
|---|---|---|
| Cardiogenic shock | Heart unable to contract efficiently, which decreases the amount of circulating blood | Heart failure, myocardial infarction, arrhythmias, cardiomyopathy, cardiac tamponade |
| Distributive shock | Systemic vasodilation | Sepsis, anaphylaxis, burns |
| Hypovolemic shock | Loss of blood volume | Hemorrhage, dehydration |
| Neurogenic shock | Inability to maintain heart rate and blood pressure | Central nervous system injury (brain or spinal cord) |
Source: THIS TUTORIAL HAS BEEN ADAPTED FROM “CLINICAL NURSING SKILLS” BY Christy Bowen at OpenStax. ACCESS FOR FREE AT https://openstax.org/books/clinical-nursing-skills/pages/1-introduction. LICENSING: CREATIVE COMMONS ATTRIBUTION 4.0 INTERNATIONAL.
REFERENCES
AdventHealth. (2025, March 20). How to Differentiate an Annual Wellness Visit vs. Physical Exam. AdventHealth Primary Care+. How to Differentiate an Annual Wellness Visit vs. Physical Exam | AdventHealth Primary Care+
Physical Exam. (2023, April 14). Cleveland Clinic. Physical Examination: What Is a Physical Exam?
Weighing In on ”Don’t Weigh Me” Cards. (2025). Scripps Health. Weighing the Pros and Cons of 'Don't Weigh Me' Cards - Scripps Health
Wong, B. (2022, January 19). PSA: You Probably Don’t Need to Be Weighed at the Doctor’s Office. HuffPost. PSA: You Probably Don't Need To Be Weighed At The Doctor's Office | HuffPost Life
Torrey, T. (2025, March 17). Do Patients Have the Right to Refuse Medical Treatment? Verywell Health. Do Patients Have the Right to Refuse Treatment?
Eustice, C. (2025). Crepitus Causes and Treatments. Verywell Health. Crepitus: Crackling in a Joint or the Lungs
Nichol JR, Sundjaja JH, Nelson G. Medical History. [Updated 2024 Apr 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK534249/
Goldberg, C. (n.d.). Write Ups. U.C. San Diego School of Medicine Practical Guide to Clinical Medicine. UC San Diego's Practical Guide to Clinical Medicine
What Is White Coat Syndrome? (2022, August 3). Cleveland Clinic. What Is White Coat Syndrome?