Table of Contents |
Throughout this course, you have learned about the many challenges in the field of public health encounters while practitioners aim to help diverse populations achieve optimal health. Ideally, the future of public health would ensure a system that is resilient when taxed by overwhelming challenges and that focuses on preventing and proactively predicting illness at the community level rather than providing reactive care when someone becomes ill (Betts et al., 2021). You have already learned a great deal about many of the challenges, and there are too many to focus on in this lesson. What follows is a deeper dive into a few that, if addressed in the future, could significantly improve public health and the quality of life for the populations served. This list is not exhaustive, and certainly other areas need improvement to enhance public and community health along with those listed in the following sections.
Among the many challenges facing public and community health, funding is often the priority issue that prevents quality services from reaching the intended audiences. There are several economic challenges that could impact public and community health in the future.
EXAMPLE
Economic downturns can lead to budget cuts, reducing the resources available for health initiatives. Funding shortages mean that public health programs that often rely on government funding are in an unpredictable situation. Economic factors can influence the availability of health care professionals. Low wages and poor working conditions can lead to a shortage of doctors, nurses, and other health care workers.EXAMPLE
Other workforce challenges are as follows:In the absence of funding, the existing health programs may struggle to maintain quality and accessibility. Without funding, marginalized communities will face even greater barriers. Insufficient funding can stifle innovation in health care. New technologies, treatments, and preventive measures may not be developed or implemented, hindering progress in public health. Public health funding is also highly dependent on the federal, state, and local political administration at the time and their agenda. At one end, some administrations and agendas support and nurture public health efforts and increase funding, programs, and jobs; at the opposite end, some political administrations and agendas can oppose and undermine public health efforts and initiate sharp cuts to funding, programs, and jobs. This will be briefly discussed further in the next section, “Policy.” Reimagining funding, which is addressed a bit more later in this lesson, for public and community health is crucial to ensure the well-being of all individuals to build resilient health systems for the future.
Much of how public and community health functions is predicated on understanding bureaucratic delays related to creating and implementing public health policies. These processes are slow, which can delay the necessary health interventions and responses to emerging health threats. Health policies can be influenced by political agendas, which may not always align with the best interests of public health. This can lead to policies that prioritize political gains over health outcomes. Policymakers often must make tough decisions about how to allocate limited resources. This can result in some health programs being underfunded or neglected.
IN CONTEXT
Medicaid Expansion Proposed in the Affordable Care Act (ACA)
In the previous section, we introduced the fact that public health funding is extremely reliant on the political environment, which can change significantly as leadership changes. The policies of any given administration, whether at the federal, state, and/or local level, can dramatically influence whether public health efforts survive, thrive, or fail.
Recall from an earlier lesson that the ACA proposed that the Medicaid program be expanded at the state level to cover more Americans. Prior to Medicaid expansion through the ACA, Medicaid was primarily for children, those with disabilities, and adults with median income levels at or below 65% of the federal poverty level.
Medicaid expansion began in 2014 and extended coverage to include nonelderly adults with incomes up to 133% of the federal poverty level. Depending on the policies of their political administrations over time, some states’ governors, such as Michigan and New Hampshire, opted into the expansion right away.
Other states’ governors, such as those from North Carolina and South Dakota, waited longer until 2023, which delayed coverage on Medicaid to qualified residents in those states. Ten states, including Florida and Texas, have not opted into Medicaid expansion at all. Since the inception of the Medicaid expansion, over 18.6 million people have newly enrolled in Medicaid due to the expanded eligibility granted by their government’s administration. States that expanded Medicaid have seen greater progress in reducing the uninsured rate among low-income adults than states that did not expand.
Medicaid expansion allows more low-income individuals to gain health insurance coverage. This includes adults without dependent children who were previously ineligible. With Medicaid coverage, newly insured individuals can access preventive services such as vaccinations, screenings, and regular checkups, which help in the early detection and management of health conditions. Without Medicaid expansion in some states, the residents of these states most likely continue to be uninsured.
(Congressional Research Service, 2021; Harker & Sharer, 2024; Office of the Assistant Secretary for Planning and Evaluation, 2024)
Policies can sometimes create regulatory barriers that make it difficult for health care providers to deliver services efficiently. For example, overly strict regulations can limit the availability of certain treatments or medications like treatments for opioid use disorder (OUD). Although they are considered the gold standard treatment, access to these medications remains limited due to stringent regulations. For instance, only about one in four people living with an OUD receive targeted medication-based treatment (e.g., buprenorphine or methadone; R Street, 2023). These regulations can include restrictions on prescribing practices, limits on the number of patients a doctor can treat with these medications, and extensive paperwork requirements (Miron et al., 2019).
New health policies can face resistance from the public, especially if they are perceived as restrictive or infringing on personal freedoms (e.g., stay-at-home orders to prevent disease transmission, mask mandates, vaccination requirements for the school environment, and controlling the sale and possession of firearms). This can hinder the implementation and effectiveness of these policies. Policies that do not take into account the diverse needs of different communities can exacerbate health inequities. For example, a one-size-fits-all approach may not address the unique health challenges faced by marginalized groups like a disaster preparedness policy that depends on people driving to shelters when not all people are mobile or have cars; a policy that requires them to leave their pets behind; or a national weight loss program that doesn’t factor in different cultural norms like ethnic food preferences, body image perspectives, or the ability to afford certain foods.
A workforce shortage in public and community health can have a significant impact on the future of public health. Recall from earlier in the course that some reasons for the public health workforce shortage relate to the hardships (like burnout) faced during the COVID-19 pandemic; many people retire, management lacks succession planning to replace those that do retire, and new graduates may find higher wages in the for-profit sector. Fewer health care professionals mean longer wait times for patients and limited availability of services. This can lead to delayed diagnoses and treatments, worsening health outcomes. Other public health activities are also affected by a shortage, like community collaboration; health education and promotion; health literacy efforts; outreach to vulnerable communities; securing or diversifying additional funding sources; and assessment, monitoring, and evaluation efforts.
Existing health care workers may face increased workloads, leading to burnout and decreased quality of care. Overworked staff are more likely to make errors, which can negatively affect patient safety. Preventive care, such as vaccinations and screenings, may be deprioritized due to staff shortage. This can result in higher rates of preventable diseases and conditions.
Workforce shortages can exacerbate health disparities, particularly in underserved communities. These areas may already have limited access to health care, and a shortage of providers can further restrict access to essential services.
Both health care and public health workers and patients can experience increased stress and mental health issues due to workforce shortages. Health care workers may face emotional exhaustion, while patients may feel anxious about their ability to receive timely care. In times of crisis, such as pandemics or natural disasters, a robust health care workforce is crucial for an effective response. Shortages can hinder the ability to manage and mitigate public and community health emergencies.
IN CONTEXT
Exhausted Health Care Workers
The COVID-19 pandemic took a heavy toll on health care and public health professionals, leading to widespread exhaustion and burnout. One notable case study involves health care workers at two Swedish hospitals. During the first wave of the pandemic, one in five health care workers reported high burnout symptoms. These symptoms persisted throughout the crisis, with high levels of burnout and depressive symptoms observed up to a year later (Appelbom et al., 2024).
Another study highlighted the emotional exhaustion experienced by U.S. health care workers. The survey included over 15,000 physicians, 11,000 nurses, and more than 5,000 other clinical staff. Approximately 50% of all respondents reported burnout, with the highest levels among nurses (56%) and other clinical staff (54.1%; Rotenstein et al., 2023).
These studies underscore the immense strain placed on health care workers during the pandemic and the need for better support systems to address their mental health and well-being. The pandemic has shown that health care systems must be prepared to support their workforce during crises to ensure both the well-being of health care professionals and the quality of patient care.
Burnout can lead to decreased quality of care, as exhausted health care professionals are more likely to make errors and less likely to provide compassionate care. Shortages can limit essential health services, particularly in underserved areas. Preventive services, such as vaccinations and screenings, may be deprioritized, leading to higher rates of preventable diseases.
To shape the future of public and community health and improve the quality of care, several key strategies are listed below and should be considered.
IN CONTEXT
Strategies for Building Resilient Communities
Addressing workforce shortages and burnout is crucial. This includes offering competitive salaries, improving working conditions, providing mental health support for public health workers, and carrying out succession planning as retirees leave the public health workforce (Minemyer, 2018).
Ensuring that all communities, especially marginalized ones, have equitable access to health care services improves public and community health. This can be achieved through policies that address social determinants of health (SDoH) and reduce health disparities.
Emphasizing preventive care to reduce the burden of chronic disease promotes healthier lifestyles. This includes increasing access to vaccinations and regular health screenings and promoting exercise and healthier eating habits, to name a few preventive measures.
Leveraging technology to enhance health care delivery means more access to care for some populations. Telemedicine, electronic health records, and future use of AI-driven diagnostics can improve efficiency and patient outcomes. For example, CDC’s Data Modernization project is a $1 billion project focused on upskilling (learning new skills or improving existing ones to stay current and competitive in a rapidly changing world) the public health workforce, facilitating data sharing, and improving surveillance since data are our most powerful tool in public health. Therefore, modernizing our data systems grows more urgent as health challenges evolve (CDC, 2024).
Involving communities in health planning and decision-making processes ensures that health programs are tailored to the specific needs of the population.
Reimagining funding models, as mentioned earlier, can ensure sustainable and adequate resources for public health programs. This includes exploring public–private partnerships and innovative financing mechanisms.
Strengthening public health systems to be better prepared for emergencies means building more robust infrastructure, training health care workers, conducting robust evaluations of programs and services to strengthen the evidence base used to justify continued funding for the sustainability of programs and services, and developing rapid response strategies to address public health crises.
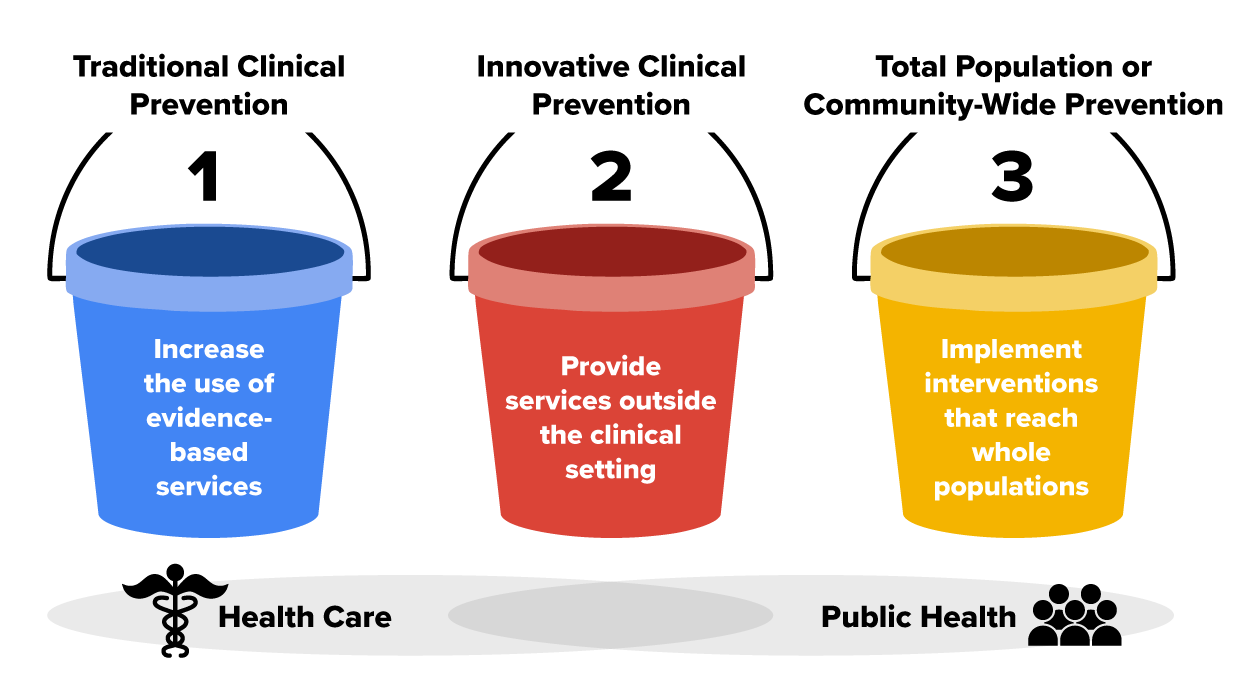
The CDC Public Health 3.0 model and many other evidence-based strategies proposed by professionals and researchers alike suggest the future of public health should emphasize a cross-sector collaboration and data-driven decision-making approach. The following table lists the components of such an approach that are key to enhancing public and community health.
| The CDC Public Health 3.0 Model | |
|---|---|
| Component Name | Description |
| Strong leadership and workforce | Public health leaders acting as chief health strategists and guiding efforts across multiple sectors to address social, environmental, and economic conditions that impact health |
| Strategic partnerships | Collaborating with and across various sectors, including government, private, and nonprofit organizations, to create a unified approach to public health |
| Flexible and sustainable funding | Developing innovative funding models that blend public and private resources to support public health initiatives |
| Timely and locally relevant data, metrics, and analytics | Utilizing real-time data and advanced analytics to inform public health strategies and measure outcomes |
| Enhanced foundational infrastructure | Strengthening the infrastructure needed to support public health activities, including technology, facilities, and workforce development |
(DeSalvo et al., 2017)
This image depicts the concepts behind the CDC’s Public Health 3.0 approach to the future of public health.
 Others (besides the CDC) have conceptualized the future of public and community health by infusing the components from Public Health 3.0 with some out-of-the-box thinking. Six dimensions of this new vision for public health encompass similar components and suggest that we view the public health landscape as an ecosystem with dimensions that are mutually reinforcing. The components include public health investment as a well-established business imperative, wherein public health agencies do not necessarily need to be at the center of all the innovation. Ecosystem partners (e.g., public health agencies working with private and nonprofit sectors) should do all the work toward unified goals (Betts et al., 2021).
Others (besides the CDC) have conceptualized the future of public and community health by infusing the components from Public Health 3.0 with some out-of-the-box thinking. Six dimensions of this new vision for public health encompass similar components and suggest that we view the public health landscape as an ecosystem with dimensions that are mutually reinforcing. The components include public health investment as a well-established business imperative, wherein public health agencies do not necessarily need to be at the center of all the innovation. Ecosystem partners (e.g., public health agencies working with private and nonprofit sectors) should do all the work toward unified goals (Betts et al., 2021).

To address the funding issues previously mentioned, some suggestions for innovation in funding are included in the table below.
| Innovation Ideas | Example |
|---|---|
| Streamlining of funding sources to remove what is now a patchwork of funding resources | Private equity funding is utilized, that is, investors put their money into private health care companies to help them grow. |
| Social impact investing | People put their money into projects or companies that aim to make a positive difference in society. |
| Establishment of public health trusts | These organizations manage funds and resources to improve the health of communities. |
| Community development financial institutions (CDFIs) | These specialized organizations provide financial services to underserved markets and populations and capital to support health programs, infrastructure, and services in low-income and underserved areas. |
| Social and governance investments |
People put their money into companies that do good things for the planet and society. Governance refers to running a fair and honest company with good leadership and transparency. |
Ways to also address funding issues include public health leaders leveraging what is already available like Medicaid waivers, workplace wellness efforts, and understanding and capitalizing on future investment models that could promote health. Medicaid waivers refer to special permission from the government to allow states to try new ways of providing health care to people who need it. Normally, Medicaid has strict rules about what services can be offered and who can get them. But with a waiver, states can test out different programs and services to see if they work better for their residents. It’s all about finding new and better ways to help people stay healthy.
Finally, to address workforce shortages, it is suggested that the future of the public health workforce should be more resilient, multidisciplinary, and robust, including being racially and ethnically diverse with skills that include training in data science (e.g., disease surveillance data, analyzing health trends data, resource allocation distribution based upon data, program evaluation data, and risk assessment data) and being better able to communicate concepts of public health to anyone. Public health should also be included in K–12 education on career paths so that interest can be explored and started early (Betts et al., 2021).
Innovation is a game changer for the future of public and community health. It allows us to tackle unmet health needs in new and effective ways. Innovative practices can improve the efficiency and quality of health care services.
EXAMPLE
Telemedicine has made it easier for people to access health care without leaving their homes.Social innovation involves the community in health initiatives, making them active participants rather than passive recipients. Innovation encourages collaboration between different groups and sectors to address complex health challenges. By embracing innovation and other approaches to the future of public health, more resilient and effective public health systems can be created to meet the needs of all communities.
Source: THIS TUTORIAL WAS AUTHORED BY SOPHIA LEARNING. PLEASE SEE OUR TERMS OF USE.
Disclaimer: The use of any CDC and United States government materials, including any links to the materials on the CDC or government websites, does not imply endorsement by the CDC or the United States government of us, our company, product, facility, service, or enterprise.
REFERENCES
Appelbom, S., Nordström, A., Finnes, A., Wicksell, R. K., & Bujacz, A. (2024). Healthcare worker burnout during a persistent crisis: A case–control study. Occupational Medicine, 74(4), 297–303. doi.org/10.1093/occmed/kqae032
Betts, D., Gordon, R., Cruse, C. B., & Egizi, A. M. (2021, November 29). The future of the public’s health. Reimagining the health ecosystem: Programs, policies, and systems for strengthening public health. Deloitte Insights. www2.deloitte.com/us/en/insights/industry/health-care/the-future-of-public-health.html
Centers for Disease Control and Prevention. (2024, May 15). What is data modernization? www.cdc.gov/data-modernization/php/about/index.html#:~:text=Data:%20Foundation%20of%20Public%20Health,Be%20response-ready
Congressional Research Service. (2021, June 9). Overview of the ACA Medicaid expansion. crsreports.congress.gov/product/pdf/IF/IF10399
DeSalvo, K. B., Wang, Y. C., Harris, A., Auerbach, J., Koo, D., & O’Carroll, P. (2017). Public Health 3.0: A call to action for public health to meet the challenges of the 21st century. Preventing Chronic Disease, 14, 170017. dx.doi.org/10.5888/pcd14.170017
Harker, L., & Sharer, B. (2024, June 14). Medicaid expansion: Frequently asked questions. Center on Budget and Policy Priorities. www.cbpp.org/research/health/medicaid-expansion-frequently-asked-questions-0#:~:text=Since%20the%20ACA's%20major%20coverage,(See%20Figure%201.)
Minemyer, P. (2018, January 23). Wave of baby boomer retirements could sap a quarter of the public health workforce. Fierce Healthcare. www.fiercehealthcare.com/healthcare/public-health-workforce-baby-boomers-retirement-american-journal-preventive-medicine
Miron, J., Sollenberger, G., & Nicolae, L. (2019, February 14). Overdosing on regulation: How government caused the opioid epidemic. CATO Institute. www.cato.org/policy-analysis/overdosing-regulation-how-government-caused-opioid-epidemic
Office of the Assistant Secretary for Planning and Evaluation. (2024, March 22). Health coverage under the Affordable Care Act: Current enrollment trends and state estimates. U.S. Department of Health and Human Services. aspe.hhs.gov/sites/default/files/documents/a6589500bb65294dec49d174c6ea84c1/aspe-health-coverage-under-aca.pdf
R Street. (2023, November). How red tape limits access to medications for opioid use disorder. www.rstreet.org/wp-content/uploads/2023/11/FINAL2-opioid-explainer-11-23.pdf
Rotenstein, L. S., Brown, R., Sinsky, C., & Linzer, M. (2023). The association of work overload with burnout and intent to leave the job across the healthcare workforce during COVID-19. Journal of General Internal Medicine, 38, 1920–1927. doi.org/10.1007/s11606-023-08153-z