Table of Contents |
Medical documentation is a critical component of healthcare communication. It ensures continuity of care, supports legal and ethical standards, and facilitates accurate billing and reporting. In this lesson, you will learn about the terminology used in documentation and how to apply it correctly in clinical scenarios.
You have already learned much of the terminology that you can use in documentation. For example, you have learned abbreviations such as NPO (nothing by mouth), BID (twice a day), PRN (as needed), and QID (four times a day). In this section, you will learn about terms related to charting and documentation, as well as legal terms.
Important terms related to charting and documentation include SOAP notes, progress notes, discharge summaries, PIE notes, POMR notes, narrative notes, and EHRs (Electronic Health Records). All of these types of documentation can be used in a wide variety of settings, including outpatient facilities, inpatient facilities, emergency departments, and rehabilitation and long-term care.
IN CONTEXT
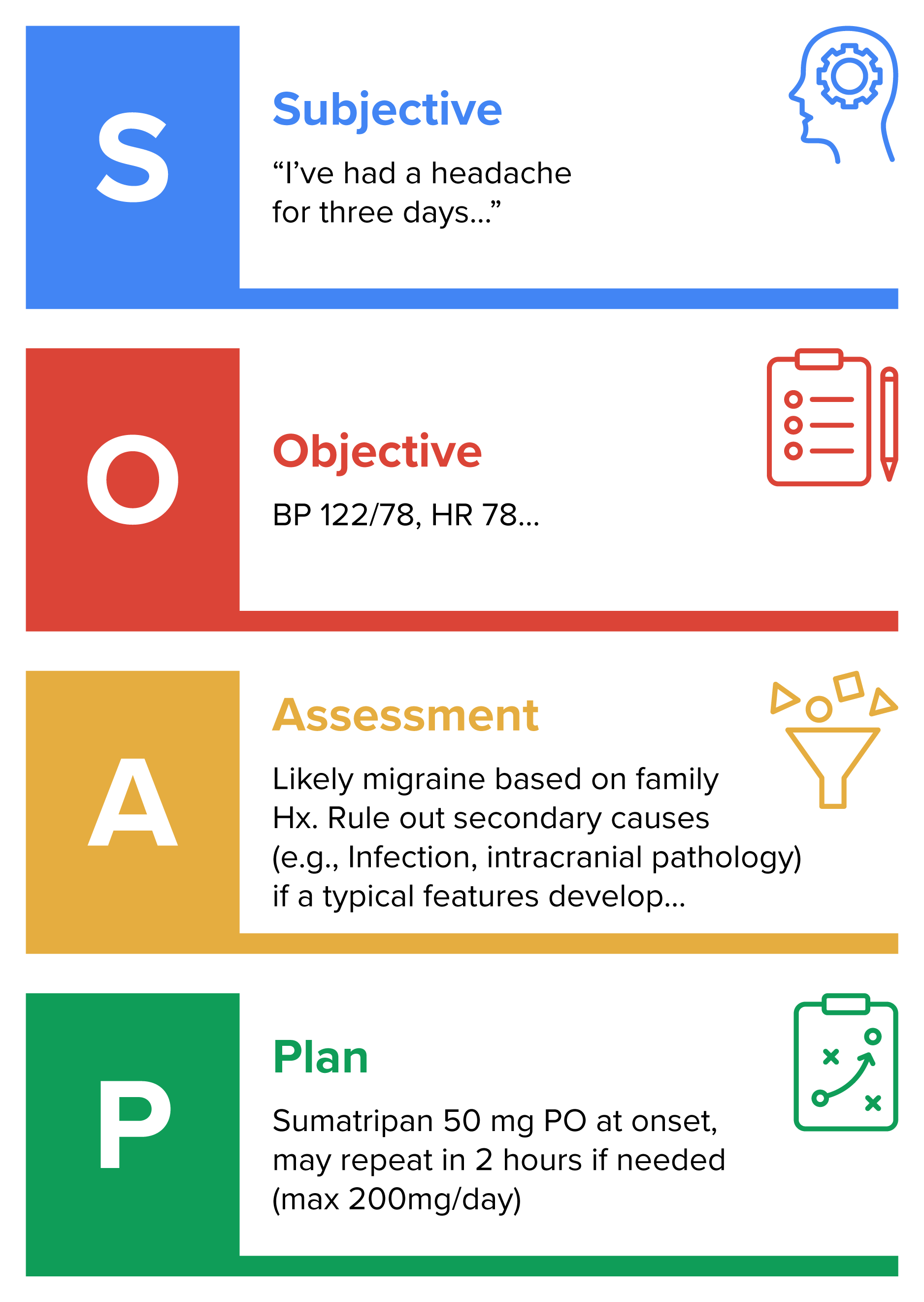
The Four Key Components of a SOAP Note
S – Subjective
This section includes what the patient reports. This includes symptoms, concerns, and history from the patient’s perspective. Common elements include the chief complaint (CC; e.g., “I’ve had a headache for three days.”), history of present illness (HPI), review of systems (ROS), and past medical, surgical, family, and social history. It is important to review and list all patient complaints, not just the one that has brought the patient to this clinical encounter (Podder et al., 2023).
O – Objective
This section includes what the clinician observes or measures. This includes physical exam findings, vital signs, and diagnostic data. Common elements include vital signs (e.g., BP, HR, Temp, RR), physical exam findings (e.g., “Tenderness in RUQ”), and any test data (e.g., results from laboratory testing and imaging).
A – Assessment
This section includes the clinician’s interpretation. This is the medical diagnosis or differential diagnosis based on the subjective and objective data. Examples include:
Note that the assessment should include the differential diagnosis. This means that the clinician should list possible diagnoses to be considered, with the rationale for which is most likely and which is unlikely. If there are diagnoses that are particularly concerning, even if unlikely, this is the place to mention them so that others can be aware of the possibility (Podder et al., 2023).
- “Likely viral upper respiratory infection”
- “Rule out appendicitis”
- ICD-10 codes may be included for billing/documentation
P – Plan
This section presents the next steps in care. This outlines treatment, further testing, referrals, and patient education. Common elements include medications prescribed, imaging or laboratory testing ordered, follow-up instructions, and lifestyle or dietary recommendations.
The acronym OLDCARTS can be used to remember important components of the HPI. This acronym stands for onset, location (in the body), duration, characterization, alleviating and aggravating factors, radiation (whether the problem is in one place or moves), temporal factor (does the problem vary in severity at certain times of day), and severity (on a scale of 1 to 10; Podder et al., 2023).
The order of the sections can be rearranged as needed to draw attention to important information. In some cases, the format APSO can be useful to quickly draw attention to the possible diagnosis and plan of treatment (Podder et al., 2023).
It is also important to keep SOAP notes clear and short to make important information easy to find (Podder et al., 2023), as shown in the example below.
A medical progress note is a daily or episodic documentation written by healthcare providers to track a patient's clinical status, response to treatment, and overall progress during care. It’s a cornerstone of inpatient and outpatient medical records. The purposes of a progress note include monitoring changes in symptoms, physical findings, or lab results, communicating updates between providers across shifts or specialties, supporting clinical decisions and justifying interventions, and documenting continuity of care for legal, billing, and quality assurance. Progress notes are often presented in SOAP note format, described below.
You have previously encountered discharge summaries. A medical discharge summary is a formal document prepared when a patient is released from a healthcare facility, such as a hospital, rehabilitation center, or skilled nursing facility. It serves as a comprehensive record of the patient’s stay and provides essential information for follow-up care.
The purposes of a discharge summary include communicating the course of treatment and outcomes to outpatient providers, ensuring continuity of care and safe transitions, and supporting billing, legal documentation, and quality assurance.
The key components of a discharge summary include patient information (such as name, age, sex, medical record number, admission date, and discharge date); reason for admission (such as the chief complaint or diagnosis), the hospital course (including a summary of clinical findings, procedures, treatments, and progress), the discharge diagnosis (the final diagnosis at discharge, which may include primary and secondary conditions), medications at discharge (a list of prescribed medications with dosages and instructions), follow-up instructions (including a list of appointments, referrals, lifestyle guidance, and warning signs), and discharge disposition (meaning where the patient is going, whether home, a rehabilitation facility, a skilled nursing facility, hospice, or somewhere else).
A PIE note is a structured documentation format used primarily in nursing and some interdisciplinary settings. It stands for:
The parts are as follows. The problem clearly identifies the patient’s issue or diagnosis, often based on assessment findings or nursing diagnoses (e.g., “Acute pain related to surgical incision”). The intervention describes the actions taken to address the problem (e.g., “Administered acetaminophen 650 mg PO at 0800”). The evaluation documents the patient’s response to the intervention (e.g., “Patient reports pain decreased from 8/10 to 4/10 within 30 minutes”).

POMR refers to documentation using the problem-oriented medical record system, which was developed in the 1960s to organize patient records around specific medical problems rather than by source or chronology.
The problem-oriented medical record is a structured approach to clinical documentation that emphasizes identifying patient problems, tracking each problem individually, and promoting logical clinical reasoning.
The core components of POMR notes include the database (a comprehensive patient history, physical exam findings, lab results, and other diagnostics; this forms the foundation for identifying problems); the problem list (a numbered list of active and inactive medical issues, including diagnoses, symptoms, psychosocial concerns, and risk factors), initial plans (for each problem), and progress notes (often written in SOAP format, with each note tied to a specific problem).
For each problem, a plan (in the initial plan section) is created with:
Narrative medical notes are free-text clinical entries that describe a patient’s condition, care, and progress in a more conversational and story-like format, without rigid structure like SOAP notes. They allow healthcare providers to document observations, reasoning, and decisions in their own words.
Key features of narrative notes include an unstructured format that flows like a paragraph or story with no predefined headings; use of the clinician’s voice (reflecting the provider’s thought process, clinical judgment, and tone), an ability to capture nuances, emotional cues, and complex scenarios that structured formats might miss; and flexibility that can be useful for documenting unusual cases, psychosocial factors, or multidisciplinary care.

Electronic health records (EHRs) are ubiquitous in healthcare, replacing older paper records. These records have potential benefits of being able to contain vast quantities of data. However, there can be problems such as duplication of data. There is considerable interest in finding better ways to use EHRs, improving communication, and reducing barriers to their use (such as technical limitations and requirements for training; Tsai et al., 2020).

Documentation has important legal implications and must follow legal requirements, so there are important legal and ethical terms to know as well.
A major consideration is HIPAA, which stands for the Health Insurance Portability and Accountability Act. This is a U.S. federal law enacted in 1996. HIPAA was designed to regulate the use of identifiable health information, set standards for data security and handling, facilitate portability (maintaining insurance coverage when changing jobs), and standardize transactions (promoting uniformity in billing and administrative practices).
The Privacy Rule governs how Protected Health Information (PHI) is used and disclosed. It applies to healthcare providers, insurers, and clearinghouses and gives patients rights over their health data.
EXAMPLE
It gives patients the right to access and correct their health information.PHI is any health-related information that can identify a person, including:
- Name, address, birth date
- Medical records, lab results
- Insurance details, billing data
- Photos, biometric identifiers
The Security Rule focuses on electronic PHI (ePHI). It requires safeguards to protect PHI (administrative, physical, and technical). Examples of these safeguards include password protection, encryption, and access controls.
The Breach Notification Rule requires covered entities to notify patients and authorities of data breaches. It includes timelines and reporting requirements
The Enforcement Rule outlines penalties for non-compliance. Fines can range from hundreds to millions of dollars depending on severity.
Another important term is informed consent. This is a foundational principle in healthcare and research that ensures patients or participants understand and voluntarily agree to a proposed medical intervention, procedure, or study. Although there are certain circumstances in which informed consent may not be required (e.g., emergency interventions to save an unconscious patient’s life), informed consent is typically required for any treatment.
To be valid, informed consent must include disclosure, comprehension, voluntariness, competence, and documentation.
Disclosure requires a clear explanation of the procedure, treatment, or study. This must include the risks, benefits, and alternatives (including doing nothing), as well as an explanation of who will perform the procedure and what it involves.
Comprehension requires that the patient must understand the information. The language should be plain, avoiding medical jargon. Providers may use visual aids, interpreters, or other approaches to ensure comprehension.
Voluntariness means that the decision must be made freely, without coercion or undue influence. Patients have the right to refuse or withdraw consent at any time.
Competence means that the individual must be mentally and legally capable of making decisions. Someone may lack competence for a variety of reasons, including dementia, delirium, and intoxication. If a patient cannot consent, then a legal guardian or surrogate may provide consent.
Documentation means that consent must be documented in some way. A signed consent form is often required, especially for invasive procedures or research. In some cases, verbal consent may suffice, but it must be documented in the medical record.
Advance directives are legal documents that outline a person's preferences for medical care in case they become unable to communicate or make decisions for themselves. These documents help healthcare providers and loved ones honor the individual's wishes during critical or end-of-life situations.
EXAMPLE
Common types of advance directives include living wills, do not resuscitate (DNR) orders, and durable power of attorney for healthcare (healthcare proxy).IN CONTEXT
Examples of Advance Directives
A living will specifies which medical treatments a patient does or does not want if seriously ill or incapacitated. For example, patients can specify whether they would like the use of life-support machines (e.g., ventilators), tube feeding, or IV fluids.
A DNR, or do not resuscitate order, is a medical directive that instructs healthcare providers not to perform CPR (cardiopulmonary resuscitation) or other life-saving measures if a patient's heart stops or they stop breathing. A DNR applies to cardiac or respiratory arrest, specifically covers situations where the heart or lungs stop functioning, and typically must be signed by a physician to be valid (required in most states). Many people include a DNR in their living will or other end-of-life planning documents. A DNR does not affect other treatments; it applies only to resuscitation efforts. It does not mean the patient refuses other care like pain relief, antibiotics. DNRs are often used by patients with terminal illnesses, advanced age, or severe chronic conditions who wish to avoid aggressive interventions that may not improve quality of life.
A durable power of attorney for health care allows a patient to designate someone (a healthcare proxy) they trust to make healthcare decisions on their behalf if they are unable to make those decisions.
Advance directives can help to reduce stress and confusion for family members during emergencies, when they may have to make difficult decisions rapidly. They can be useful for anyone, not just older adults or those with serious illnesses. They’re especially important in cases of sudden accidents, strokes, or progressive conditions like dementia.
Consider the SOAP note below.
Source: THIS TUTORIAL WAS AUTHORED BY SOPHIA LEARNING. PLEASE SEE OUR TERMS OF USE.
REFERENCES
Podder V, Lew V, Ghassemzadeh S. SOAP Notes. [Updated 2023 Aug 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK482263/
Tsai, C. H., Eghdam, A., Davoody, N., Wright, G., Flowerday, S., & Koch, S. (2020). Effects of Electronic Health Record Implementation and Barriers to Adoption and Use: A Scoping Review and Qualitative Analysis of the Content. Life (Basel, Switzerland), 10(12), 327. doi.org/10.3390/life10120327
Altman, R. L., Lin, C. T., & Earnest, M. (2023). Problem-oriented documentation: design and widespread adoption of a novel toolkit in a commercial electronic health record. JAMIA Open, 6(1), ooad005. doi.org/10.1093/jamiaopen/ooad005
Vtaylor. (n.d.). What is the difference between informed and implied consent? Raynes and Lawn, Trial Lawyers. rayneslaw.com/what-is-the-difference-between-informed-and-implied-consent/
Merriam-Webster. (n.d.). Photophobia. In Merriam-Webster.com dictionary. Retrieved September 27, 2025, from www.merriam-webster.com/dictionary/photophobia