Table of Contents |
The birth of a child marks the end of pregnancy and the beginning of a new set of responsibilities that includes feeding the newborn. Before the end of pregnancy, a woman needs to consider whether to feed her infant breast milk, infant formula, or both.
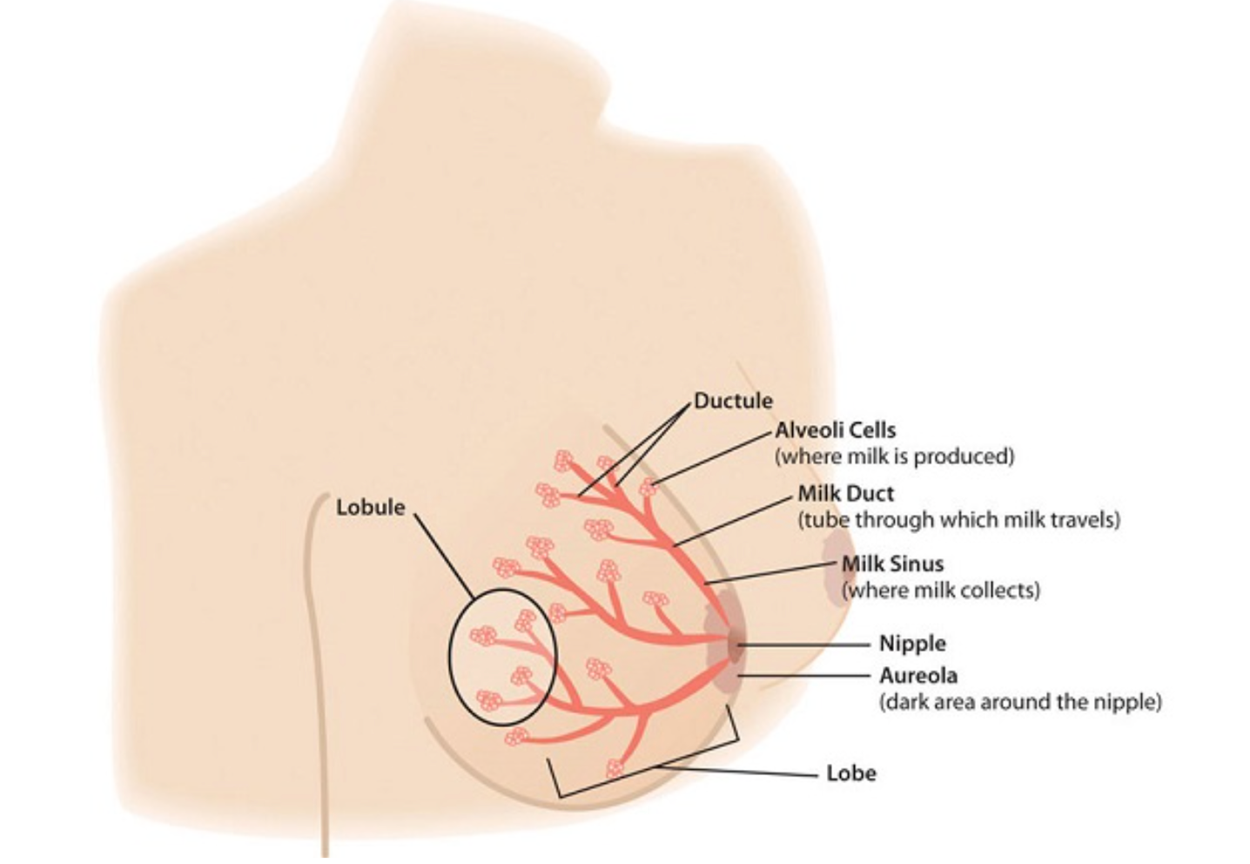
Lactation is a natural process that follows pregnancy as the mammary glands secrete milk for nourishment of the infant. Mammary glands develop in a woman in puberty and remain inactive until pregnancy. During pregnancy, hormones promote the growth and development of milk-producing cells. Hormones play a major role in this, particularly during the second and third trimesters. At that point, levels of the hormone prolactin increase to stimulate the growth of the milk duct system, which initiates and maintains milk production. The hormone oxytocin causes the mammary glands to eject milk into the ducts, a response known as the let-down reflex. The mother may feel this reflex as a contraction of the breast, followed by the flow of milk and the release of pressure. However, levels of the hormone progesterone need to decrease for successful milk production because progesterone inhibits milk secretion. Shortly after birth, the expulsion of the placenta triggers progesterone levels to fall, which activates lactation.
IN CONTEXT
The alveoli cells produce milk. To secrete it, they contract and push milk into the ductules and the milk sinus, which collects the milk. When a nursing infant’s gums press on the areola and nipple, the sinuses squeeze the milk into the baby’s mouth. The nipple tissue becomes firmer with stimulation, which makes it more flexible and easier for the baby to grasp in the mouth.
After the birth of the baby, nutritional needs must be met to ensure that an infant not only survives but thrives from infancy into childhood. Breastfeeding provides the fuel a newborn needs for rapid growth and development. As a result, the World Health Organization (WHO) recommends that breastfeeding be done exclusively for the first six months of an infant’s life.
New mothers need to adjust their caloric and fluid intake to make breastfeeding possible. The RDA is 330 additional calories during the first six months of lactation and 400 additional calories during the second six months of lactation. The energy needed to support breastfeeding comes from both increased intake and from stored fat.
EXAMPLE
During the first six months after her baby is born, the daily caloric cost for a lactating mother is 500 calories, with 330 calories derived from increased intake and 170 calories derived from maternal fat stores. This helps explain why breastfeeding may promote weight loss in new mothers.Lactating women should also drink 3.1 liters of liquids per day (about 13 cups) to maintain milk production, according to the IOM. An easy guideline to remember is to drink a glass of milk, juice, or water at each meal and each time the infant nurses. As is the case during pregnancy, the RDA of nearly all vitamins and minerals increases for women who are breastfeeding their babies. The following table compares the recommended vitamins and minerals for lactating women to the levels for nonpregnant and pregnant women.
| Nutrient | Nonpregnant Women | Pregnant Women | Lactating Women |
|---|---|---|---|
| Vitamin A (mcg) | 700.0 | 770.0 | 1,300.0 |
Vitamin  (mg) (mg)
|
1.5 | 1.9 | 2.0 |
Vitamin  (mcg) (mcg)
|
2.4 | 2.6 | 2.8 |
| Vitamin C (mg) | 75.0 | 85.0 | 120.0 |
| Vitamin D (mcg) | 5.0 | 5.0 | 5.0 |
| Vitamin E (mg) | 15.0 | 15.0 | 19.0 |
| Calcium (mg) | 1,000.0 | 1,000.0 | 1,000.0 |
| Folate (mcg) | 400.0 | 600.0 | 500.0 |
| Iron (mg) | 18.0 | 27.0 | 9.0 |
| Magnesium (mg) | 320.0 | 360.0 | 310.0 |
Niacin ( ) (mg) ) (mg)
|
14.0 | 18.0 | 17.0 |
| Phosphorus | 700.0 | 700.0 | 700.0 |
Riboflavin ( ) (mg) ) (mg)
|
1.1 | 1.4 | 1.6 |
Thiamine ( ) (mg) ) (mg)
|
1.1 | 1.4 | 1.4 |
| Zinc (mg) | 8.0 | 11.0 | 12.0 |
Human breast milk not only provides adequate nutrition for infants, it also helps to protect newborns from disease. Breast milk is rich in cholesterol, which is needed for brain development.
Two to four days after birth, colostrum is replaced by transitional milk. Transitional milk is a creamy liquid that lasts for approximately two weeks and includes high levels of fat, lactose, and water-soluble vitamins. It also contains more calories than colostrum. After a new mother begins to produce transitional milk, she typically notices a change in the volume and type of liquid secreted and an increase in the weight and size of her breasts.
Mature milk is the final fluid that a new mother produces. In most women, it begins to secrete at the end of the second week post childbirth. There are two types of mature milk that appear during a feeding. Foremilk occurs at the beginning and includes water, vitamins, and protein. Hind-milk occurs after the initial release of milk and contains higher levels of fat, which is necessary for weight gain. Combined, these two types of milk ensure that a baby receives adequate nutrients to grow and develop properly.
IN CONTEXT
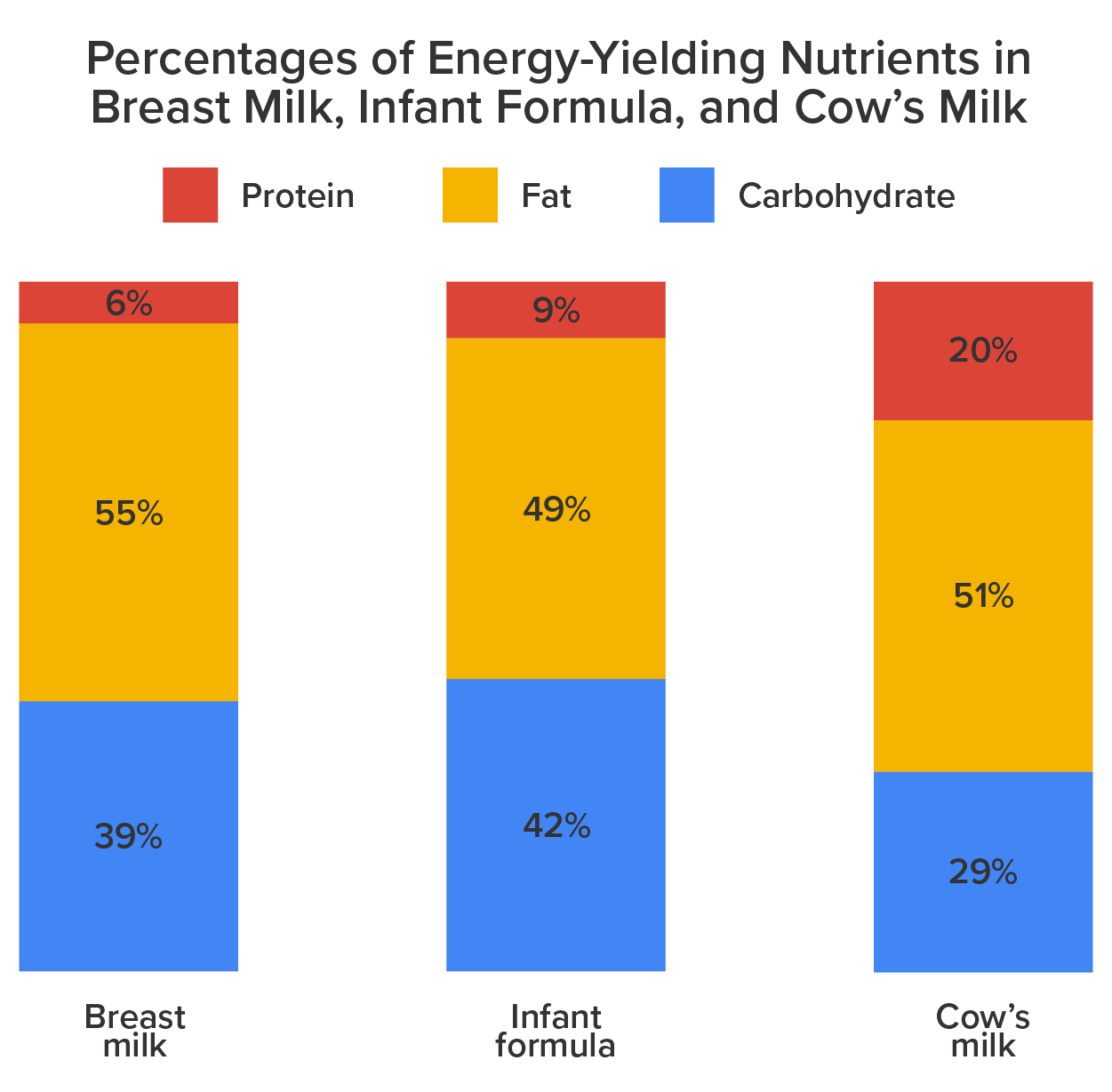
About 90 percent of mature milk is water, which helps an infant remain hydrated. The other 10 percent contains carbohydrates, proteins, and fats, which support energy and growth. Similar to cow’s milk, the main carbohydrate of mature breast milk is lactose. Breast milk contains vital fatty acids, such as docosahexaenoic acid (DHA) and arachidonic acid (ARA). In terms of protein, breast milk contains more whey than casein (which is the reverse of cow’s milk). Whey is much easier for infants to digest than casein. Complete protein, which means all of the essential amino acids, is also present in breast milk. Complete protein includes lactoferrin, an iron-gathering compound that helps to absorb iron into an infant’s bloodstream.
In addition, breast milk provides adequate vitamins and minerals. Although absolute amounts of some micronutrients are low, they are more efficiently absorbed by infants. Other essential components include digestive enzymes that help a baby digest the breast milk. Human milk also provides the hormones and growth factors that help a newborn to develop.
Breastfeeding has a number of benefits, both for the mother and for the child. Breast milk contains immunoglobulins, enzymes, immune factors, and white blood cells. As a result, breastfeeding boosts the baby’s immune system and lowers the incidence of diarrhea, along with respiratory diseases, gastrointestinal problems, and ear infections. Breastfed babies also are less likely to develop asthma and allergies, and breastfeeding lowers the risk of sudden infant death syndrome. In addition, human milk encourages the growth of healthy bacteria in an infant’s intestinal tract.
Breastfeeding has a number of other important benefits.
A maternity center can be denoted as “baby-friendly” when it does not accept substitutes to human breast milk and has implemented ten steps to support breastfeeding.
Since the BFHI began, more than fifteen thousand facilities in 134 countries, from Benin to Bangladesh, have been deemed “baby friendly.” As a result, more mothers are breastfeeding their newborns and infant health has improved, in both the developed world and in developing nations.
Although breast milk is ideal for almost all infants, there are some challenges that nursing mothers may face when starting and continuing to breastfeed their infants. These obstacles include painful engorgement or fullness in the breasts, sore and tender nipples, lack of comfort or confidence in public, and lack of accommodation to breastfeed or express milk in the workplace.
IN CONTEXT
One of the first challenges nursing mothers face is learning the correct technique. It may take a little time for a new mother to help her baby properly latch on to her nipples. Improper latching can result in inadequate intake, which could slow growth and development. However, International Board Certified Lactation Consultants (IBCLCs), obstetrical nurses, and registered dietitians are all trained to help new mothers learn the proper technique. Education, the length of maternity leave, and laws to protect public breastfeeding, among other measures, can all help to facilitate breastfeeding for many lactating women and their newborns.
Although there are numerous benefits to breastfeeding, in some cases there are also risks that must be considered. In the developed world, a new mother with HIV should not breastfeed because the infection can be transmitted through breast milk. These women typically have access to bottle formula that is safe, and can be used as a replacement for breast milk.
Women with type 1 diabetes may need careful monitoring and counseling to ensure successful lactation. These women need to adjust their energy intakes and insulin doses to meet the heightened needs of lactation.
Breastfeeding also is not recommended for women undergoing radiation or chemotherapy treatment for cancer. Additionally, if an infant is diagnosed with galactosemia, meaning an inability to process the simple sugar galactose, the child must be on a galactose-free diet, which excludes breast milk. This genetic disorder is a very rare condition, however, and only affects 1 in thirty-to sixty thousand newborns.
Most women can and should breastfeed when given sufficient education and support. However, a small percentage of women are unable to breastfeed their infants, while others choose not to. For parents who choose to bottle-feed, infant formula provides a balance of nutrients. However, not all formulas are the same, and there are important considerations that parents and caregivers must weigh.
Standard formulas use cow’s milk as a base. They have 20 calories per fluid ounce, similar to breast milk, with vitamins and minerals added. Soy-based formulas are usually given to infants who develop diarrhea, constipation, vomiting, colic, or abdominal pain, or to infants with a cow’s milk protein allergy. Hypoallergenic protein hydrolysate formulas are usually given to infants who are allergic to cow’s milk and soy protein. This type of formula uses hydrolyzed protein, meaning that the protein is broken down into amino acids and small peptides, which makes it easier to digest. Preterm infant formulas are given to low birth weight infants, if breast milk is unavailable. Preterm infant formulas have 24 calories per fluid ounce and are given until the infant reaches a desired weight.
Infant formula comes in three basic types:
IN CONTEXT
Most babies need about 2.5 ounces of formula per pound of body weight each day. Therefore, the average infant should consume about 24 fluid ounces of breast milk or formula per day. When preparing formula, parents and caregivers should carefully follow the safety guidelines since an infant has an immature immune system.
All equipment used in formula preparation should be sterilized. Prepared, unused formula should be refrigerated to prevent bacterial growth. Parents should make sure not to use contaminated water to mix formula in order to prevent foodborne illnesses.
It is important to note again that both the American Academy of Pediatrics and the WHO state that breast milk is far superior to infant formula. This table compares the advantages of giving a child breast milk to the disadvantages of using bottle formula.
| Breast Milk | Bottle Formula |
|---|---|
| Antibodies and lactoferrin in breast milk protect infants. | Formula does not contain immunoprotective factors. |
| The iron in breast milk is absorbed more easily. | Formula contains more iron than breast milk, but it is not absorbed as easily. |
| The feces that babies produce do not smell because breastfed infants have different bacteria in the gut. | The feces that bottle-fed infants produce tends to have a foul-smelling odor. |
| Breast milk is always available and is always at the correct temperature. | Formula must be prepared, refrigerated for storage, and warmed before it is given to an infant. |
| Breastfed infants are less likely to have constipation. | Bottle-fed infants are more likely to have constipation. |
| Breastfeeding ostensibly is free, though purchasing a pump and bottles to express milk does require some expense. | Formula must be purchased and is expensive. |
| Breast milk contains the fatty acids DHA and ARA, which are vital for brain and vision development. | Some formulas contain DHA and ALA. |
Source: THIS TUTORIAL HAS BEEN ADAPTED FROM LUMEN LEARNING’S “NUTRITION FLEXBOOK”. ACCESS FOR FREE AT https://courses.lumenlearning.com/suny-nutrition/. LICENSE: creative commons attribution 4.0 international.
REFERENCES
American Pregnancy Association. “Breastfeeding versus Bottle Feeding.” November 5, 2012. www.americanpregnancy.org/firstyearoflife/breastfeedingandbottle.html.
Institute of Medicine, www.iom.edu.